Maigne's Syndrome
Lumbo-Pelvic Pain Part 1
William E. Morgan
It is natural to associate the site of pain as the source of pain. If the pain is over the sacroiliac joint, it is a sacroiliac problem. If there is lateral thigh pain, it is probably a tensor fascia lata (TFL) syndrome. While pain often originates at the site of pain, other times pain is referred from another site: it is where it isn’t. This is the case with thoracolumbar junction syndrome. This malady can refer pain to the inguinal area, lateral thigh, and posterior pelvis (sacroiliac or gluteal region).
I cannot recall the number of the patients treated for TFL syndrome with foam rolling and myofascial release therapy of the lateral thigh who were finally restored to normal after an adjustment to the thoracolumbar junction. Or, additionally, how many patients had been told for years they had a sacroiliac problem and had their SI adjusted ad nauseam, but received only limited relief. However, when the thoracolumbar junction was adjusted, their pain issues resolved.
The intent of this series is to bring attention to other possible sources of pain than the most obvious. There have been many others who have written on this topic, but it deserves being resurrected every few years to keep us mindful. What I write here, and much of what has been written regarding these conditions, is based on our knowledge of anatomy and clinical observations. The astute doctor will view this and other writings on the subject through the lens of skeptical scrutiny while allowing for these clinical observations to one day be substantiated. I should note that conditions such as cluneal nerve entrapment, piriformis syndrome, and Maigne’s syndrome are primarily based on clinical observations with little firm evidence to substantiate their existence.
 Maigne's Syndrome, cluneal nerve
Maigne's Syndrome, cluneal nerve
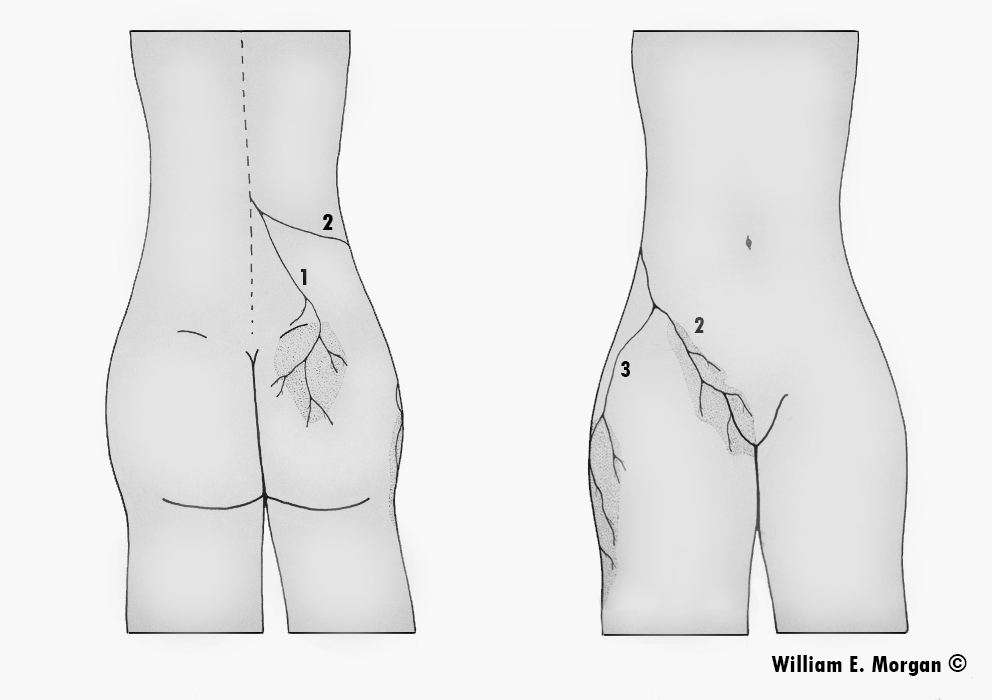
Figure 1. The thoracolumbar junction syndrome is clearly defined by a triad pattern of pain involving the posterior pelvis, lateral thigh, and inguinal region. This image identifies the distribution of pain; the posterior pelvis (1), the inguinal region (2), and the lateral thigh (3).
Maigne’s Syndrome: Thoracolumbar Junction Syndrome
Musculoskeletal providers frequently see patients with inguinal pain, sacroiliac and buttocks pain, and lateral hip pain, and it is common to focus on the region of pain rather than other possible sources of it. Pain over the sacroiliac may be interpreted as originating in the sacroiliac joint, pain in the lateral thigh as Iliotibial band syndrome, and inguinal pain as psoas dysfunction. Doctors and therapists focusing on the region of pain, manipulate the painful sacroiliac, provide foam rollers for the “Iliotibial band” pain, and perform myofascial release on the psoas muscles.
The French physician, Robert Maigne, proposed in his writings in the 1970 -80s that a thoracolumbar facet syndrome could be responsible for causing referred pain to the regions innervated by those segment’s posterior rami and the peripheral nerves which originate in that region. Maigne also proposed other techniques, such as skin rolling, to determine the tissue quality and other clinically oriented criteria which could be used to diagnose thoracolumbar syndrome. Dr. Maigne identified the syndrome which now bears his name with these observations:
- Unilateral lower back pain, usually in the sacroiliac region
- Inguinal or testicular pain
- Abdominal pain
- Gynecological symptoms or pain
- Pubic pain
Nerves Originating from the Thoracolumbar Region
The nerves which innervate the skin over the sacroiliac and buttocks (the posterior ramus of the thoracolumbar segments/cluneal nerves), the inguinal region (the posterior ramus of the thoracolumbar segments), and the lateral thigh (the posterior ramus of the thoracolumbar segments/lateral cutaneous femoral nerve) originate from the thoracolumbar junction.
It should be noted that the pain distribution may not follow standard dermatomal or peripheral nerve maps and that a sclerotomal pattern of pain (which will be a deeper pain) may be observed. Dermatome maps are general guidelines, but the actual dermatomes will vary from person to person.
 Foam roller, thoracic mobilization
Foam roller, thoracic mobilization
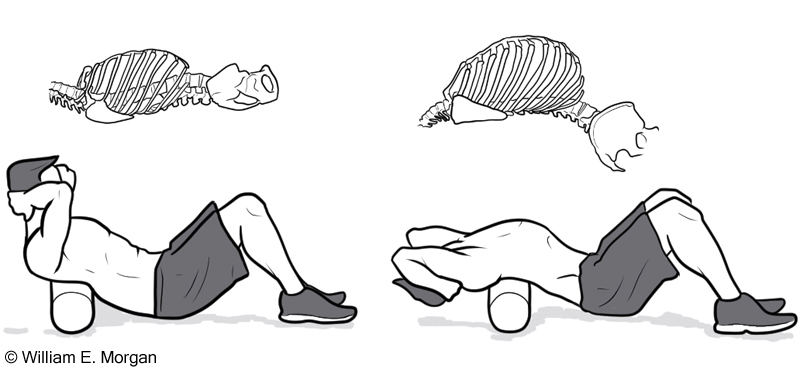
Figure 2. In addition to adjusting the thoracolumbar spine, the doctor may also prescribe a foam roller for home use. Clasp your hands behind your head with the foam roll underneath the upper portion of the thoracic spine. Extend backward over the roll while keeping the neck in a neutral posture. Repeat three or four times. Next roll the foam down the spine a few inches, and then repeat. Slowly work the foam roller down to the thoracolumbar junction.
Treatment
Maigne encouraged the use of spinal manipulation to treat this syndrome. Adjusting the lower thoracic and upper lumbar vertebrae (T10-L2) is the primary treatment. I prefer standing anterior to posterior adjustments. In addition to spinal adjustments, the patient can also self-treat at home with the use of a foam roller (figure 2).
Peripheral Nerve Entrapment
While the thoracolumbar spinal segments may be a source of pain in the inguinal region, buttocks, and lateral thigh regions as described by Maigne, there are other sources of symptoms. In subsequent articles I will address sources of nerve entrapment of the cluneal nerves, and lateral cutaneous femoral nerve, as well as conservative treatment options.
References to Doctor Maigne’s Writings:
Maigne R. - Sémiologie des dérangements intervertèbraux mineurs. Ann. Med. Phys. 1972. 15, 277-289.
Maigne R. - Dérangements intervertèbraux mineurs et syndrome cellulo-téno-myalgique. Conceptions nouvelles des mécaniques des douleurs vertébrales communes. Rev. Méditer. Sci. Méd., 1978 5, 337-348.
Maigne R. - Origine dorso-lombaire de certaines lombalgies basses. Rôle des articulations interapophysaires et des branches postérieures des nerfs rachidiens. Rev. Rhum. 1974, 41, 12, 781-789.
Maigne R. - Le syndrome de la charnière dorso-lombaire. Lombalgies basses, douleurs pseudo-viscérales, pseudo-douleurs de hanche, pseudo-tendinite des adducteurs. Sem. Hôp. Paris 1981, 57, 11-12, 545-554.
Maigne R. - Low back pain of thoracolumbar origin. Arch. Phys. Med. Rehabil. 1980, 61, 389-395.
Maigne J.Y., Lazareth J.P., Guérin-Surville H., Maigne R. - The lateral cutaneous branches of the dorsal rami of the thoraco lumbar junction. An anatomical study on 37 dissections. Surg. Radiol. Anat. 1986, 8, 251-256.
Maigne R., Le Corre F., Judet H. - Premiers résultats d’un traitement chirurgical de la lombalgie basse rebelle d’origine dorso-lombaire. Rev. Rhum. 1979, 46, 177-18.