Bone Morphology and Modic Classifications
Vertebral body edema is a common finding on MR imagery. Though degenerative changes like bony edema may seem like unimportant background noise to the busy clinician, recent studies have found that vertebral marrow edema is clinically significant and can be a progressive condition.
Michael T. Modic, MD, identified and published his findings on vertebral bony marrow changes in the journal Radiology in 1988. 1, 2 Since that time these findings and his grading criteria have borne his name. Modic changes represent MRI observations of vertebral marrow and endplate changes. These changes have been linked to trauma, disc disruption, and degeneration. More studies are currently underway to identify the clinical significance of this finding and to fully understand its progression.
The vertebral body has a dense outer barrier of cortical bone which is particularly dense at the vertebral endplates. Within this tough outer shell lies the subcortical marrow cavity. This cancellous bone is less dense and is porous. It is normal for this porous bone to contain fatty marrow. The T1 and T2 weighted MR images will reflect the presence of normal fatty marrow with a supportive bony matrix. When edema is present in the marrow, it is characterized by an influx of water content: T1-weighted images show loss of signal (hypointense signal in the marrow), while T2-weighted images will demonstrate an increased (hyperintense) signal.
Degenerative disc disease (DDD) without Modic changes is a relatively insidious and not particularly painful condition, whereas DDD with Modic changes is much more frequently associated with pain. 3,4, 5, 6, 7 Type 1 Modic changes show bony edema and inflammation and are strongly associated with back pain. Emerging evidence indicates there is a progressive nature to Modic changes. The bony edema of type I Modic changes may progress to type 2, and type 2 may progress to type 3. 8, 9, 10
Modic Types
The Modic classification system is a method for categorizing vertebral body and endplate findings on MRI. Here are the three types:
Type 1. Type 1 Modic changes are characterized by high water content that is indicative of inflammation and edema. They are manifested as hypointense (dark) on T1 weighted MRI and hyperintense (bright) on T2 weighted images.
Type 2. Modic type 2 changes identify yellow fatty infiltration into the vertebral body. On T1 images, the fatty infiltration of type 2 Modic changes will appear hyperintense, and on T2 weighted images, they will appear hyperintense or isointense.
Type 3. Modic type 3 changes are less common than types 1 and 2 with less scientific investigation. Modic type 3 is identified by decreased signal or hypointense on both T1 and T2 weighted MR images. These findings can typically be correlated with sclerosis on plain film x-ray.
Conclusion
Modic changes can have strong clinical significance. Type 1 Modic changes have been strongly associated with [deep bony] pain and inflammation where type 2 and type 3 Modic Changes are less likely to be associated with refractory pain and tend to be more stable.
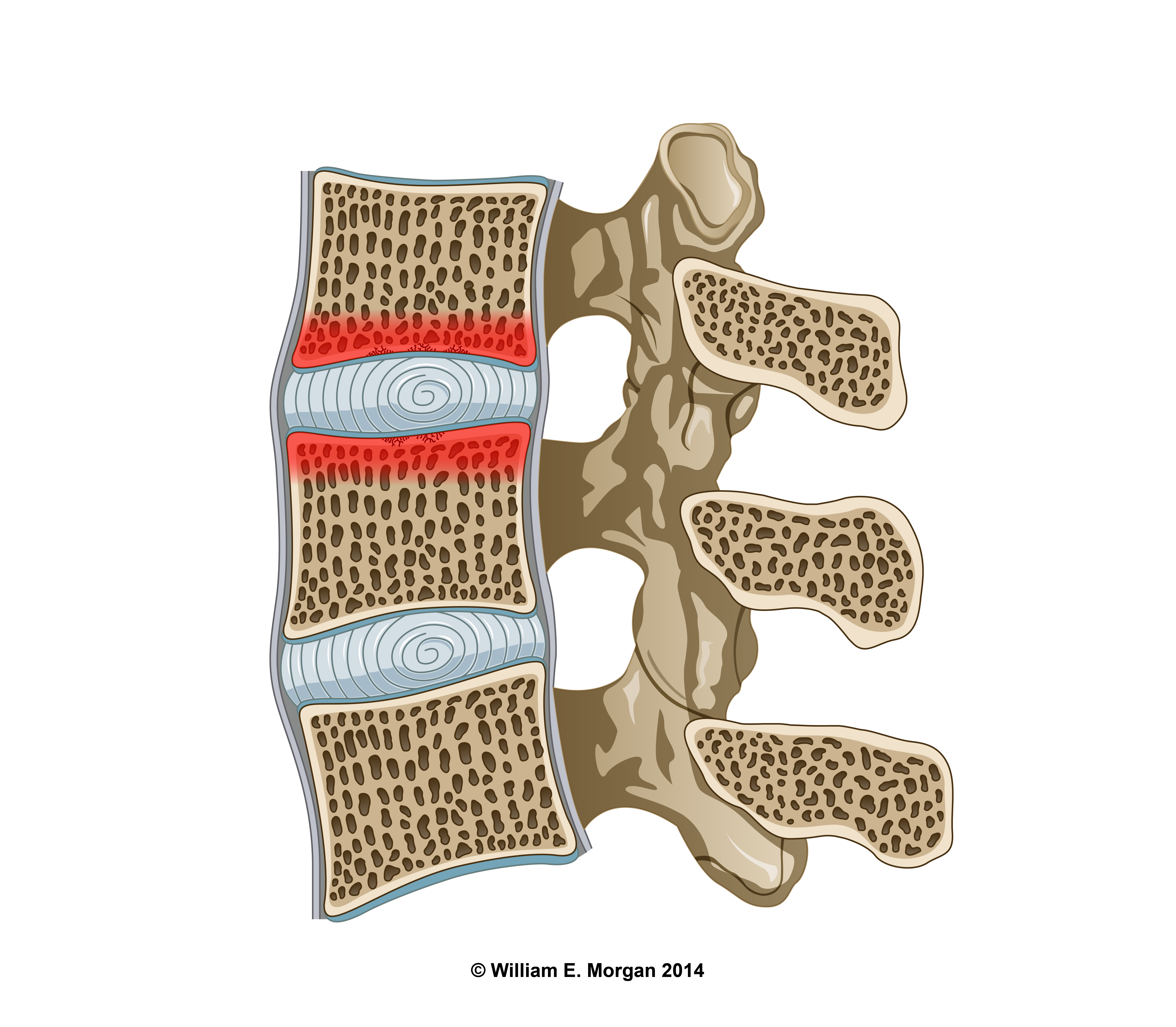 Bony edema (red) extending into the spongy subcortical bone.
Bony edema (red) extending into the spongy subcortical bone.
Image 1. Bony edema (red) extending into the spongy subcortical bone.
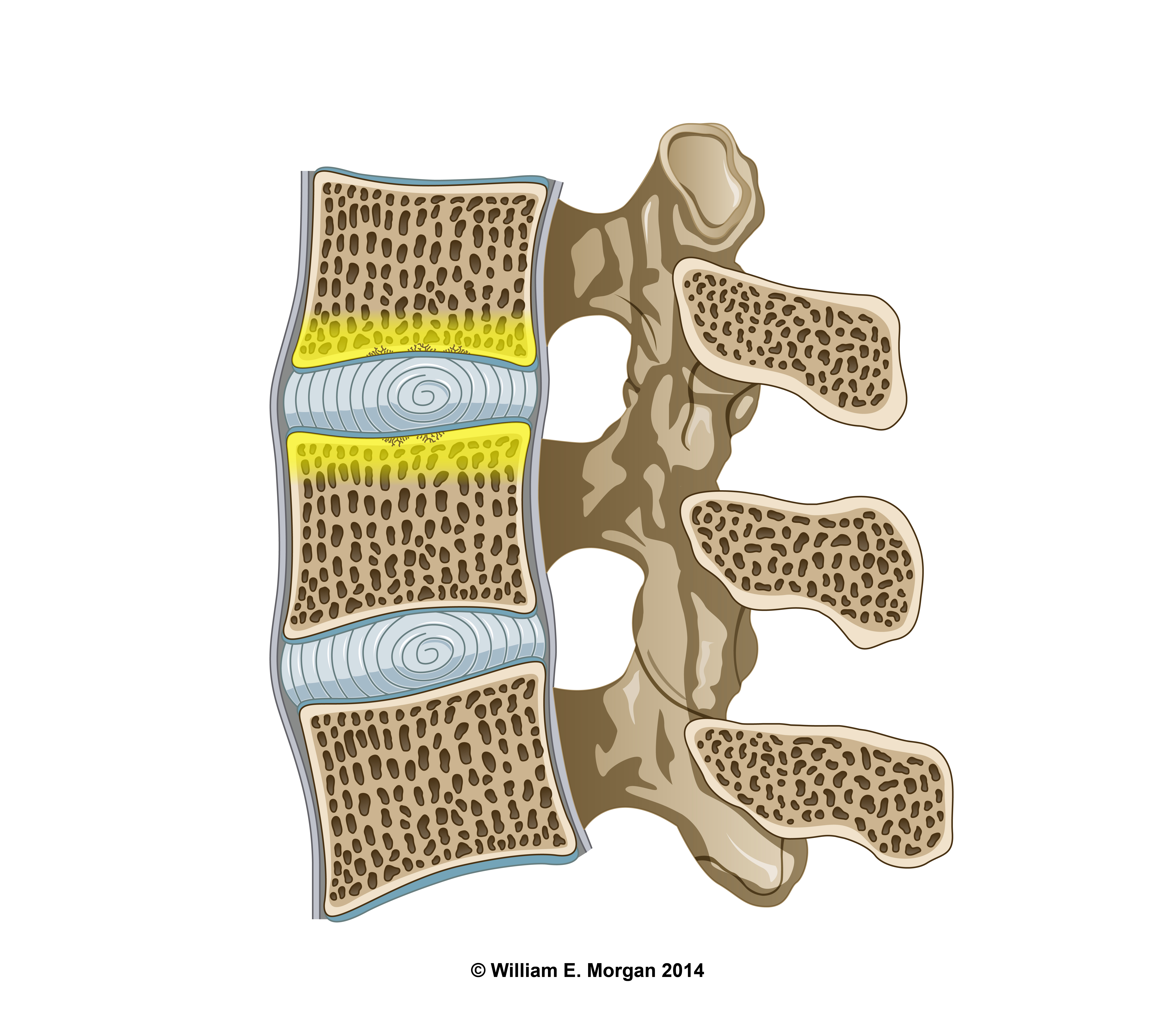 Type 2 Modic changes
Type 2 Modic changes
Image 2. Yellow fatty infiltration of the subcortical bone is characteristic of Modic 2 changes.
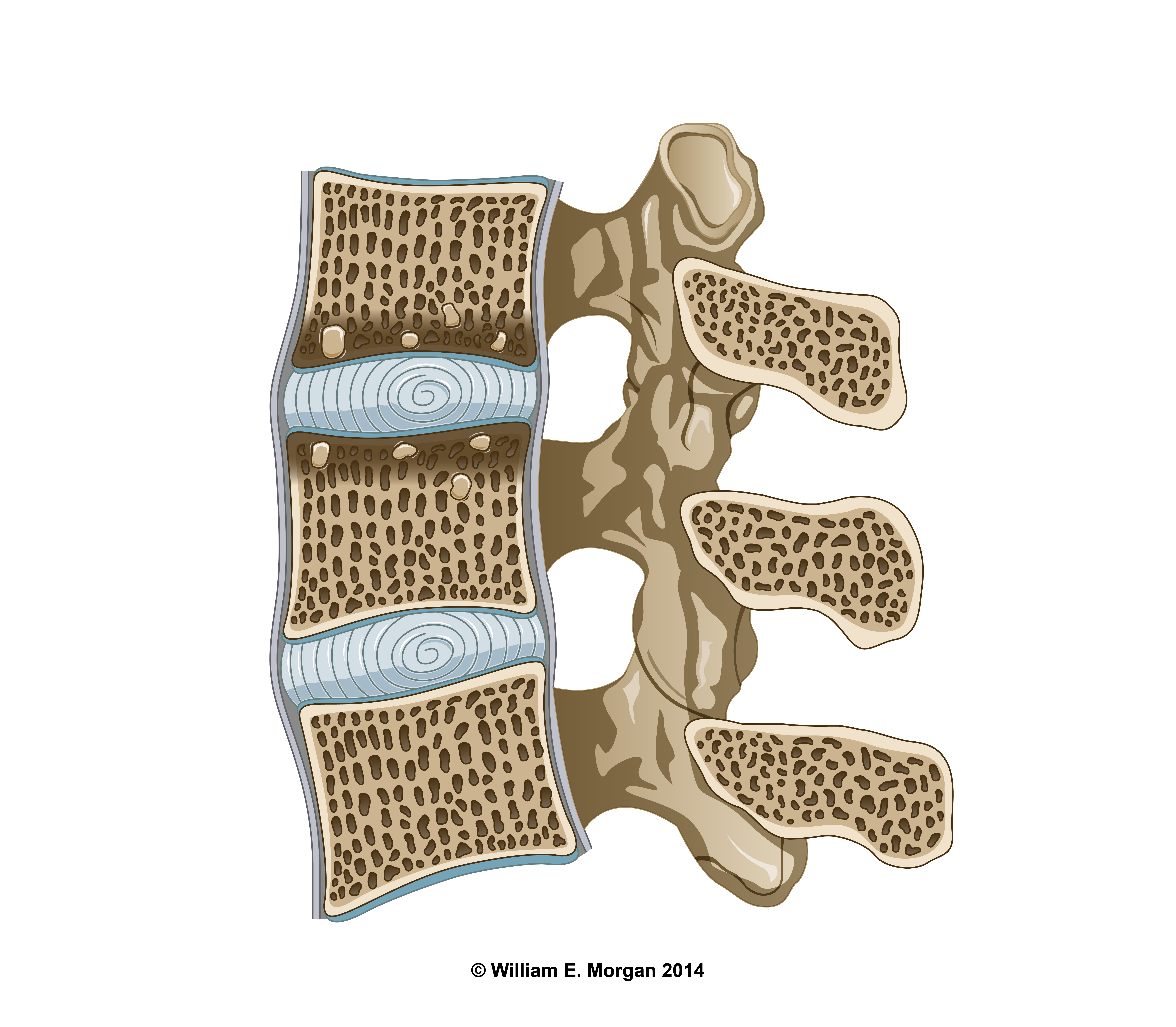 Sclerotic changes of the cortical bone and thickening of the endplates are indicative of Modic 3 changes.
Sclerotic changes of the cortical bone and thickening of the endplates are indicative of Modic 3 changes.
Image 3. Sclerotic changes of the subcortical bone and thickening of the vertebral endplates. Type 2 and type 3 changes are normally associated with progressive DDD.
http://www.amazon.com/William-Morgan/e/B00KNACR7G/ref=sr_ntt_srch_lnk_5?qid=1451756945&sr=1-5