Caring for Patients with Amputations (Part one of a series)
With hundreds of chiropractors working in the VA and DOD healthcare systems along with an increasing number of veterans entering the civilian sector of healthcare it is very likely that chiropractors will contribute to the multidisciplinary care of war-wounded amputees. We should be well versed in the unique neurological and physiological nuances associated with amputations as well as with the mechanical changes which accompany them.
In addition to war-wounded amputees, there has been a dramatic increase in adult-onset diabetes in the United States and Mexico, which is another major cause of amputations. This series will introduce practitioners to the unique complications which accompany amputations. This first article will introduce the phenomenon known as Phantom Limb Pain. The attempt to understand this condition has led to increased knowledge in treating many types of pain and a deeper understanding of neuroplasticity.
Phantom limb pain (the perception of pain, paresthesia, itching, tingling, and other sensations of a missing limb) occurs in more than 90% of those who have lost a limb to amputation.1 This phenomenon has been documented for centuries in medical textbooks and in literature. While the perception of phantom limb pain may be a mild painless annoyance to some, in others it is very disruptive and interferes with work or sleep. Phantom limb pain is a hallucination created in the subconscious mind that a missing limb still exists. This hallucination involves a very realistic perception of the missing limb even though the conscious mind clearly conceptualizes the lost limb.
Particularly interesting is that phantom limb pain has been noted in those who are missing limbs due to birth defects.2 People who never had a limb can still have the perception of phantom limb pain. This points to the prospect that the brain is disposed to an interaction with its limbs. The brain is hardwired to send and receive neurotransmissions with the various body parts. The perception of having limbs is implanted into the brain rather than learned. In response to this knowledge, Ronald Melzack introduced the concept of the presence of a neuromatrix. 1
The Neuromatrix
The neuromatrix theory states that pain is not produced from passive recognition of nociception, but rather by an aggregate of the central nervous system, the brain and spinal cord, actively working together to generate the perception of pain. The neuromatrix may or may not actively produce pain based on nociception and many other factors. The neuromatrix may produce pain when there is not significant amounts of nociceptive input. We see this in phantom limb pain, complex regional pain syndrome, and other chronic pain syndromes. There are other times when little or no pain is perceived although there is a significantly large amount of nociceptive input. For example, in the heat of battle it is common for troops to receive wounds that would normally be very painful, yet they do not feel the pain. The brain apparently recognizes that the distraction of pain in a crisis could compromise the individual’s ability to overcome the immediate threat and could result in death. Therefore the input of nociception is ignored by the brain and pain is not perceived. The brain actively prioritizes survival over localized tissue preservation. It chooses not to produce the perception of pain.
Key points:
- Tissue damage does not cause pain. It may result in the transmission of nociceptive impulses, but it does not directly cause pain.
- The central nervous system (brain and spinal cord) produces the perception of pain. This is often an interpretation of nociceptive input, but not always.
- Nociception and pain are not the same thing.
- Production of the perception of pain is a neurologically active phenomenon, not a passive one.
The Homunculus
Homunculus literally means “little man” in Latin. The brain has been mapped out as a blueprint in the cortical homunculus. There are two renditions of the cortical homunculus: the somatosensory and the motor. In the somatosensory homunculus we see that certain parts of the brain are responsible for the innervation of certain parts of the body (figure 1, left image). Note that the hand and arm occupy a significantly large portion of the homunculus. In the case of an upper extremity amputation (figure 1, right image), there is a large portion of the brain once designated to innervate the arm, but it has no arm with which to interact. There is a vacuum of interaction, a void. Nature abhors a vacuum. So the neuromatrix fills the “vacuum” by actively creating the missing perceptions and sensations that the arm may feel, resulting in phantom limb pain.
In the absence of sensory input from a limb, as seen in the amputation of a limb, the brain creates its own sensory input to satisfy its need to account for that body part. These manufactured sensations may be the perception of warmth or cold, itchiness, achiness, or pain, sometimes severe refractory pain. Phantom limb pain can be incapacitating and disruptive to sleep, work, and relationships.
In addition to phantom limb pain, patients with amputations can also experience hypersensitivity of the adjoining body parts within the somatosensory homunculus. When looking at the somatosensory homunculus (figure 1, left image) the face is located next to the upper extremity, and the genitals are located next to the leg. Following an amputation, the portion normally designated to account for the upper extremity melds with the portion which normally accounts for the face. A missing leg might meld with the portion which normally accounts for the genitals. This can result in altered sensations and increased sensitivity of the neighboring body parts in the homunculus. For example, a patient with a missing arm may experience hypersensitivity or pain in the face and jaw. A patient with a leg amputation may experience hypersensitivity or pain of the genitals. This was demonstrated when Ramachandran used light stimulation of patients’ faces with a Q-tip to produce the perception of sensations in the missing limb.3 The neurological complications of amputation combined with the more obvious and visually apparent consequences of a lost limb (stump care, prosthetics, wheelchairs, ambulation, and activities of daily living) can prove very disruptive to patients.
There is a strong connection between the brain’s awareness of the body and sight. The brain coordinates its perception of self through the combined senses of proprioception and sight. When there is conflict between what the brain expects to see, proprioception, and the reality of a missing limb, phantom limb pain can occur.4 Recognizing the distinct visual association between the brain and the neuromatrix and how strongly the interactive sense of self responds to visual cues, researchers sought to develop a non-pharmaceutical treatment for phantom limb pain. Ramachandran and colleagues identified the contribution of sight to phantom limb pain and devised a novel treatment for phantom limb pain: Mirror Therapy. The next installment in this series will introduce Mirror Therapy as an effective non–pharmaceutical treatment of phantom limb pain.
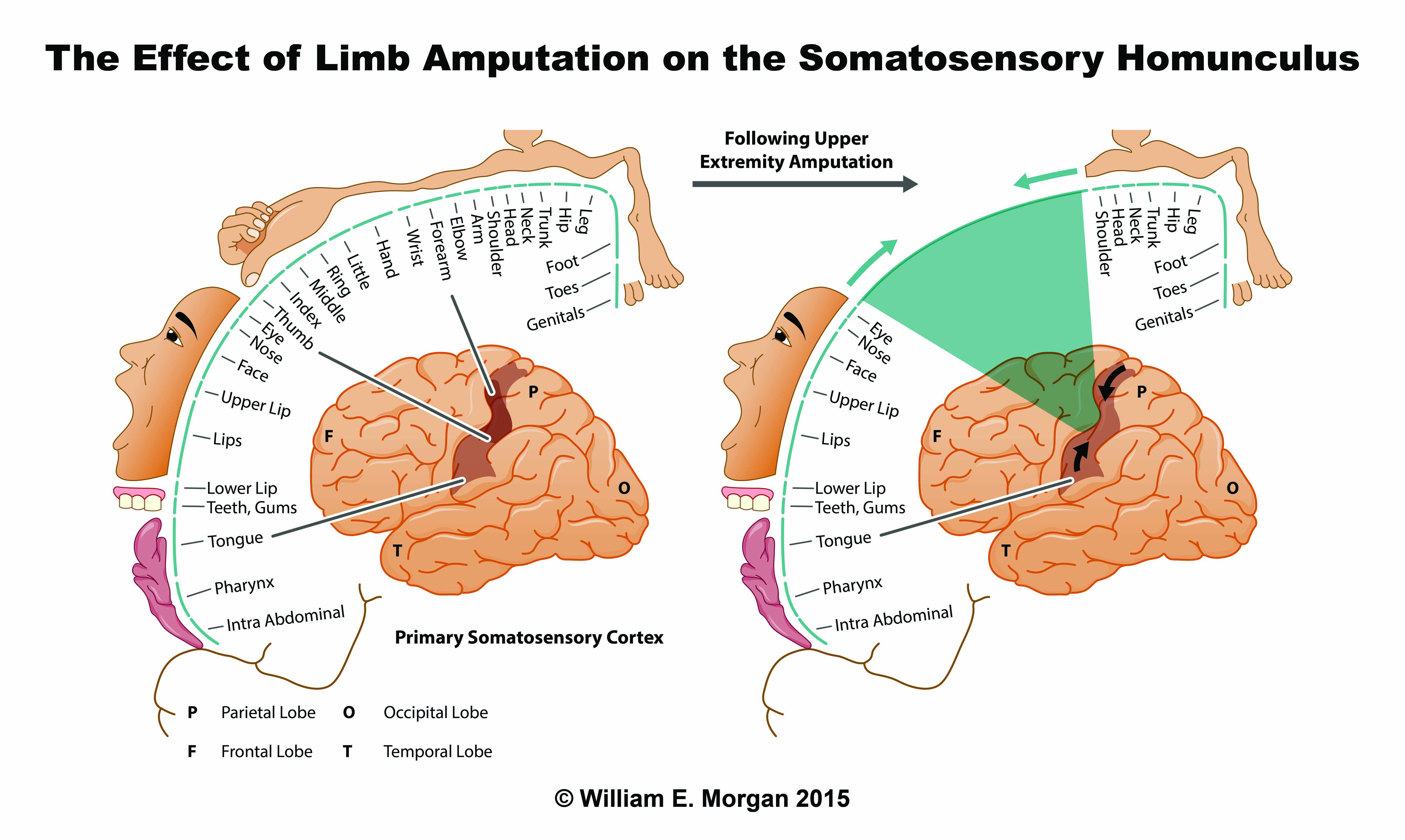
Figure 1. These schematics of the somatosensory homunculus attempt to illustrate and map the regions of the brain responsible for interpreting the sensory input from various portions of the brain. The image on the left illustrates an intact somatosensory homunculus. Note the large amount of the homunculus that the upper extremity occupies. The image on the right illustrates the void that is formed in the brain when an amputation occurs.
Disclaimer
The views expressed in this article are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of the Army, Department of Defense, nor the U.S. Government.
1 Melzack R. Phantom limbs and the concept of a neuromatrix. Trends Neurosci 1990;13:88-92.
2 Melzack R, Israel R, Lacroix R, Schultz G. Phantom limbs in people with congenital limb deficiency or amputation in early childhood. Brain. 1997 Sep;120 ( Pt 9):1603-20.
3 Ramachandran VS, Rogers‐Ramachandran D, Cobb S. Touching the phantom limb. Nature 1995; 377: 489–90.
4 Ramachandran VS, Hirstein W. The perception of phantom limbs. Brain 1998;121:1603-1630